
XYLISOL
LAVAJE NASAL
EL ALIADO IDEAL EN LA PREVENCIÓN Y TRATAMIENTO DE RINITIS ALÉRGICA Y SINUSITIS CRÓNICA



SPRAY CONTINUO SIN
IMPORTAR LA POSICIÓN
XYLISOL LAVAJE NASAL
- Inhibe el crecimiento y la adherencia bacteriana.
- Inhibe la formación de biofilms rinosinusales responsables de la cronicidad de las infecciones de las vías respiratorias. Se ha demostrado su efecto sobre el biofilm en 3 especies bacterianas sinonasales: Staphylococcus aureus, Staphylococcus epidermidis, Pseudomonas aeruginosa.
- Regula la concentración del óxido nítrico presente en los senos paranasales, favoreciendo su actividad antiviral y antibacteriana, pudiendo controlar así el desarrollo de la rinosinusitis crónica.
- Mejora significativamente los síntomas de la rinosinusitis crónica comparado a lavajes de solución salina isotónica.
INDICACIONES
Coadyuvante en el tratamiento y la prevención de rinosinusitis, adenoiditis, otitis, amigdalitis, laringitis y faringitis.
Higiene nasofaríngea. Favorece la eliminación del moco, evitando la retención de secreciones nasales. Elimina alérgenos por arrastre previniendo Rinitis Alérgicas.
Útil en caso de inflamación de cuerdas vocales con y sin disfonía y tos de naturaleza irritativa.
Alivio total de los síntomas nasales del resfrío y gripe.
Post-operatorio de
la cirugía nasal.
ESTUDIOS CLÍNICOS

The in vitro effect of xylitol on chronic rhinosinusitis biofilms.
Jain R, Lee T, Hardcastle T, Biswas K, Radcliff F, Douglas R. Rhinology.
2016 Dec 1;54(4):323-328. doi: 10.4193/Rhino15.380.
Biofilms have been implicated in chronic rhinosinusitis (CRS) and may explain the limited efficacy of antibiotics.
There is a need to find more effective, non-antibiotic based therapies for CRS. This study examines the effects of xylitol on CRS biofilms and planktonic bacteria.
Xylitol in preventing acute otitis media.
Uhari M, Tapiainen T, Kontiokari T.
Vaccine. 2000 Dec 8;19 Suppl 1:S144-7. doi: 10.1016/s0264-410x(00)00294-2.
Xylitol is a polyol sugar alcohol and is referred to as birch sugar, because it can be produced from birch. Natural sources of xylitol include plums, strawberries, raspberries and rowanberries. Xylitol inhibits the growth of Streptococcus pneumoniae and it inhibits the attachment of both pneumococci and Haemophilus influenzae on the nasopharyngeal cells. In two clinical trials xylitol was found efficient to prevent the development of acute otitis media with a daily dose of 8.4–10 g of xylitol given in five divided doses. The efficacy in these 2–3 months follow-up trials was 40% when chewing gum was used and 30% with xylitol syrup.
The need to use antimicrobials reduced markedly when using xylitol. In a high-risk group of children with tympanostomy tubes xylitol was ineffective in preventing otitis. Xylitol appears to be an attractive alternative to prevent acute otitis media. A more practical frequency of doses should be found before its use can be widely recommended. © 2000 Elsevier Science Ltd. All rights reserved.
The osmolyte xylitol reduces the salt concentration of airway surface liquid and may enhance bacterial killing.
Zabner J, Seiler MP, Launspach JL, Karp PH, Kearney WR, Look DC, Smith JJ, Welsh MJ.
Proc Natl Acad Sci U S A. 2000 Oct 10;97(21):11614-9. doi: 10.1073/pnas.97.21.11614. PMID: 11027360.
The thin layer of airway surface liquid (ASL) contains antimicrobial substances that kill the small numbers of bacteria that are constantly being deposited in the lungs. An increase in ASL salt concentration inhibits the activity of airway antimicrobial factors and may partially explain the pathogenesis of cystic fibrosis (CF). We tested the hypothesis that an osmolyte with a low transepithelial permeability may lower the ASL salt concentration, thereby enhancing innate immunity. We found that the five-carbon sugar xylitol has a low transepithelial permeability, is poorly metabolized by several bacteria, and can lower the ASL salt concentration in both CF and non-CF airway epithelia in vitro. Furthermore, in a double-blind, randomized, crossover study, xylitol sprayed for 4 days into each nostril of normal volunteers significantly decreased the number of nasal coagulase-negative Staphylococcus compared with saline control. Xylitol may be of value in decreasing ASL salt concentration and enhancing the innate antimicrobial defense at the airway surface.
Xylitol nasal irrigation in the treatment of chronic rhinosinusitis.
Lin L, Tang X, Wei J, Dai F, Sun G.
Am J Otolaryngol. 2017 Jul-Aug;38(4):383-389. doi: 10.1016/j.amjoto.2017.03.006. Epub 2017 Apr 4.
Objective: To evaluate the efficacy of xylitol nasal irrigation (XNI) treatment on chronic rhinosinusitis (CRS) and to investigate the effect of XNI on nasal nitric oxide (NO) and inducible nitric oxide synthase (iNOS) mRNA in maxillary sinus. Materials and methods: Patients with CRS were enrolled and symptoms were assessed by Visual Analog Scale (VAS) and Sino-Nasal Outcome Test 22 (SNOT-22). Nasal NO and iNOS mRNA in the right maxillary sinus were also examined. Then, they were treated with XNI (XNI group) or saline nasal irrigation (SNI, SNI group) for 30 days, after which their symptoms were reassessed using VAS and SNOT-22, and nasal NO and iNOS mRNA in the right maxillary sinus were also reexamined. Results: Twenty-five out of 30 patients completed this study. The scores of VAS and SNOT-22 were all reduced significantly after XNI treatment, but not after SNI. The concentrations of nasal NO and iNOS mRNA in the right maxillary sinus were increased significantly in XNI group. However, significant changes were not found after SNI treatment. Furthermore, there were statistical differences in the assessments of VAS and SNOT-22 and the contents of nasal NO and iNOS mRNA in the right maxillary sinus between two groups. Conclusions: XNI results in greater improvement of symptoms of CRS and greater enhancement of nasal NO and iNOS mRNA in maxillary sinus as compared to SNI.
Nitric oxide in the nasal airway: a new dimension in otorhinolaryngology.
Djupesland PG, Chatkin JM, Qian W, Haight JS.
Am J Otolaryngol. 2001 Jan-Feb;22(1):19-32. doi: 10.1053/ajot.2001.20700.
The discovery that the gas nitric oxide (NO) is an important signaling molecule in the cardiovascular system earned its Nobel prize in 1998. NO has since been found to play important roles in a variety of physiologic and pathophysiologic processes in the body including vasoregulation, hemostasis, neurotransmission, immune defense, and respiration.
The surprisingly high concentrations of NO in the nasal airway and paranasal sinuses has important implications for the field of otorhinolaryngology. NO provides a first-line defense against micro-organisms through its antiviral and antimicrobial activity and by its upregulation of ciliary motility. Nasal treatments such as polypectomy, sinus surgery, removal of hypertrophic adenoids and tonsils, and treatment of allergic rhinitis may alter NO output and, therefore, the microbial colonization of the upper airways. Nasal surgery aimed at relieving nasal obstruction may do the same but would also be expected to improve pulmonary function in patients with asthma and upper airway obstruction.
NO output rises in a number of conditions associated with chronic airway inflammation, but not all of them. Concentrations are increased in asthma, allergic rhinitis, and viral respiratory infections, but reduced in sinusitis, cystic fibrosis, primary ciliary dysfunction, chronic cough, and after exposure to tobacco and alcohol. Therefore, NO, similar to several other inflammatory mediators, probably subserves different functions as local conditions dictate. At present, it seems that the measurement of NO in the upper airway may prove valuable as a simple, noninvasive diagnostic marker of airway pathologies.
The objective of this review is to highlight some aspects of the origin, physiology, and functions of upper airway NO, and to discuss the particular methodological problems that result from the complex anatomy.
(Am J Otolaryngol 2001;22:19-32. Copyright © 2001 by W.B. Saunders Company).
Xylitol nasal irrigation in the management of chronic rhinosinusitis: a pilot study.
Weissman JD, Fernandez F, Hwang PH.
Laryngoscope. 2011 Nov;121(11):2468-72. doi: 10.1002/lary.22176. Epub 2011 Oct 12. Erratum in: Laryngoscope. 2012 Nov;122(11):2611.
Objectives/Hypothesis: To determine the tolerability of xylitol mixed with water as a nasal irrigant and to evaluate whether xylitol nasal irrigation results in symptomatic improvement of subjects with chronic rhinosinusitis.
Study Design: A prospective, randomized, double-blinded, controlled crossover pilot study.
Methods: Twenty subjects were instructed to perform sequential 10-day courses of daily xylitol and saline irrigations in a randomized fashion, with a 3 day washout irrigation rest period at the start of each treatment arm. Collected data included patient characteristics, along with Sino-Nasal Outcome Test 20 (SNOT-20) and Visual Analog Scale (VAS) scores reported at the beginning and end of each irrigation course.
Results: Fifteen of the 20 subjects (75%) returned their SNOT-20 and VAS data for analysis. There was a significant reduction in SNOT-20 score during the xylitol phase of irrigation (mean drop of 2.43 points) as compared to the saline phase (mean increase of 3.93 points), indicating improved sinonasal symptoms (P ¼ .0437). There was no difference in VAS scores.
No patient stopped performing the irrigations owing to intolerance of the xylitol, although its sweet taste was not preferred by three subjects (21%). One patient reported transient stinging with xylitol.
Conclusions: Xylitol in water is a well-tolerated agent for sinonasal irrigation. In the short term, xylitol irrigations result in greater improvement of symptoms of chronic rhinosinusitis as compared to saline irrigation.
ROL DEL BIOFILM DE STAPHYLOCOCCUS AUREUS EN LA RINOSINUSITIS CRÓNICA
Varios procesos inmunopatológicos con inflamación persistente en la superficie de la mucosa conducen a rinosinusitis crónica (CRS). Estudios recientes informaron que la colonización nasal por Staphylococcus aureus (SA) se detectó en el 67% de los pacientes. Se han reportado diferentes factores etiológicos como la biopelícula de S. aureus y sus productos secretados. En particular, las enterotoxinas de S. aureus (SE), principalmente Enterotoxina B (SEB). Se reportó IgE específica contra las SE en casi la mitad de los tejidos nasales homogeneizados a partir de pólipos nasales. La sensibilización a las enterotoxinas estafilocócicas (SE) se correlacionó con la gravedad de la rinosinusitis crónica eosinofílica (ECRS).
S. aureus secreta además un grupo de exoproteínas, como exotoxinas y enzimas, que convierten los tejidos del huésped en los nutrientes necesarios para el crecimiento bacteriano. La toxina α de S. aureus (hemolisina-α) es el principal agente citotóxico liberado, y representa la primera exotoxina bacteriana formadora de poros en ser identificada. La formación de poros en las membranas de las células huésped susceptibles altera los gradientes de iones, compromete la integridad de la membrana, activa las vías de señalización del estrés y provoca la muerte celular. S. aureus libera también diferentes exotoxinas que son capaces de funcionar como superantígenos (SAG). Los SAG son exotoxinas altamente mitogénicas que desencadenan un estímulo enormemente poderoso para los linfocitos T.
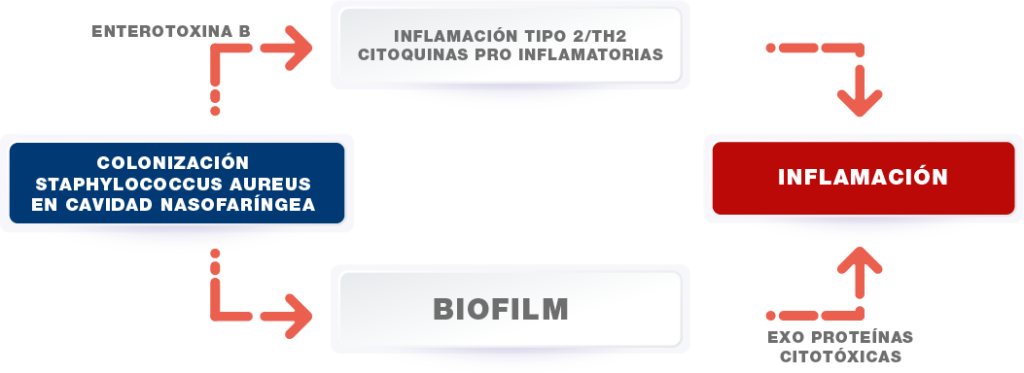
Las exoproteínas secretadas por el biofilm de S. aureus son citotóxicas para la barrera epitelial nasal humana en la rinosinusitis crónica desempeñando un papel importante en la etiopatogenia del CRS. La destrucción de la integridad de la mucosa se informó como uno de los principales mecanismos patogénicos.
ESTUDIOS CLÍNICOS
The role of Staphylococcus aureus enterotoxin B in chronic rhinosinusitis with nasal polyposis.
Zahra Chegini, Mojtaba Didehdar, Amin Khoshbayan, Jafar Karami4,5, Milad Yousefmashouf6 and Aref shariati.
Chegini et al. Cell Communication and Signaling (2022) 20:29. https://doi.org/10.1186/s12964-022-00839-x
CRS with nasal polyps (CRSwNP) is a multifactorial disease, and various etiological factors like bacterial superantigens are known to develop this disease. Recent studies reported that Staphylococcus aureus nasal colonization was detected in 67% of the patients with CRSwNP. Moreover, it was reported that specifc IgE against S. aureus enterotoxins are discovered in almost half of the nasal tissue homogenates from nasal polyps. Thus, investigations have highlighted the role of staphylococcal enterotoxins, especially enterotoxin B (SEB), in pathogenesis of CRSwNP. The destruction of mucosal integrity was reported as a main SEB-related pathogenic mechanisms in CRSwNP. SEB activates Toll Like Receptor 2 and triggers the production of pro-infammatory cytokines; furthermore, it induces reactive oxygen species and endoplasmic reticulum stress-induced infammation that may cause epithelial cell integrity disruption and enhance their permeability. SEB-induced Type 2/Th2 pathway results in degranulation of eosinophils, cationic proteins production, and localized eosinophilic infammation. Furthermore, SEB may be involved in the expression of RORC and HIF-1α in Tregs and by maintaining the infammation in sinonasal mucosa that could have a main role in the pathogenesis of nasal polyposis. Diferent in vitro fndings were confrmed in animal studies; however, in vivo analysis of SEB-induced nasal polyps and CRS remains unfulflled due to the lack of appropriate animal models.
Finally, after elucidating diferent aspects of SEB pathogenesis in CRSwNP, therapeutic agents have been tested in recent studies with some encouraging results. The purpose of this article is to summarize the most important fndings regarding SEB-induced CRS and nasal polyposis.
Staphylococcus aureus biofilm exoproteins are cytotoxic to human nasal epithelial barrier in chronic rhinosinusitis.
Beula Subashini Panchatcharam, MBBS, MD, Clare M. Cooksley, PhD, Mahnaz Ramezanpour, PhD, Rajan Sundaresan Vediappan, MBBS, DLO, MS, Ahmed Bassiouni, MBBS, PhD, Peter J. Wormald, MD, FRACS, Alkis J. Psaltis, MBBS, FRACS, PhD and Sarah Vreugde, MD, PhD.
Panchatcharam BS, Cooksley CM, Ramezanpour M, et al. Staphylococcus aureus biofilm exoproteins are cytotoxic to human nasal epithelial barrier in chronic rhinosinusitis. Int Forum Allergy Rhinol. 2020;00:1-13. Received: 27 November 2019; Revised: 22 February 2020; Accepted: 26 March 2020. DOI: 10.1002/alr.22566.
Background: Chronic rhinosinusitis patients (CRS) suffer from chronic inflammation of the sinus mucosa associated with chronic relapsing infections. Mucosal biofilms, associated with Staphylococcus aureus, have been implicated as a cause. We compared the effect of exoproteins secreted from clinical isolates of S aureus from CRS patients in planktonic and biofilm form on the nasal epithelial barrier. Methods: Clinical S aureus isolates from 39 CRS patients were grown in planktonic and biofilm forms and their exoproteins concentrated. These were applied to primary human nasal epithelial cells grown at the air-liquid interface. Transepithelial electrical resistance, permeability of flourescein isothiocyanate-dextrans, and cytotoxicity were measured. Structure and expression of tight junctions zona occludens-1, and claudin-1 proteins were assessed by electron microscopy and immunofluorescence. The Wilcoxon signed rank test was used for statistical analyses. Results: S aureus biofilm exoproteins showed dose- and time-dependent reduction of transepithelial electrical resistance, increased cell toxicity, and increased permeability (p < 0.001) compared with equal concentrations of planktonic cultures. Discontinuity in zona occludens-1 and claudin-1 immunofluorescence was confirmed as disrupted tight junctions on electron microscopy. Conclusion: S aureus biofilm exoproteins disrupt the mucosal barrier structure in a time- and dose-dependent manner and are toxic. Damage to the mucosal barrier by S aureus biofilm exoproteins may play a major role in CRS etiopathogenesis. C 2020 ARS-AAOA, LLC.
Chronic Rhinosinusitis, S. aureus Biofilm and Secreted Products, Inflammatory Responses, and Disease Severity.
Gohar Shaghayegh, Clare Cooksley, Mahnaz Ramezanpour, Peter-John Wormald, Alkis James Psaltis and Sarah Vreugde.
Citation: Shaghayegh, G.; Cooksley, C.; Ramezanpour, M.; Wormald, P.-J.; Psaltis, A.J.; Vreugde, S. Chronic Rhinosinusitis, S. aureus Biofilm and Secreted Products, Inflammatory Responses, and Disease Severity. Biomedicines 2022, 10, 1362. https://doi.org/10.3390/ biomedicines10061362. Academic Editor: Célia F. Rodrigues. Received: 10 May 2022. Accepted: 6 June 2022. Published: 9 June 2022. Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Chronic rhinosinusitis (CRS) is a persistent inflammation of the nasal cavity and paranasal sinuses associated with tissue remodelling, dysfunction of the sinuses’ natural defence mechanisms, and induction of different inflammatory clusters. The etiopathogenesis of CRS remains elusive, and both environmental factors, such as bacterial biofilms and the host’s general condition, are thought to play a role. Bacterial biofilms have significant clinical relevance due to their potential to cause resistance to antimicrobial therapy and host defenses. Despite substantial medical advances, some CRS patients suffer from recalcitrant disease that is unresponsive to medical and surgical treatments.
Those patients often have nasal polyps with tissue eosinophilia, S. aureus-dominant mucosal biofilm, comorbid asthma, and a severely compromised quality of life. This review aims to summarise the contemporary knowledge of inflammatory cells/pathways in CRS, the role of bacterial biofilm, and their impact on the severity of the disease. Here, an emphasis is placed on S. aureus biofilm and its secreted products. A better understanding of these factors might offer important diagnostic and therapeutic perceptions for recalcitrant disease.